The NIHR HRC Network Collaboration Challenge Fund (CCF) provides targeted pump-priming funding (up to £50,000) to catalyse cross-HRC collaborations involving at least 3 HRCs per project. CCF is centered around 4 aims:
-
Generating preliminary evidence in under-researched areas
-
Driving methodological innovation
-
Supporting proof-of-concept developments
-
Producing policy-relevant insights
These activities are intended to strengthen collaborative research across the HRC Network, enhance its collective impact, and generate the evidence and partnerships needed to secure larger external funding opportunities.
Transparent and rigorous assessment and review process
-
Initial eligibility screening confirms the required participation by at least 3 HRCs, budget compliance, project timelines, and other core requirements.
-
Review window comprises of independent and peer reviewers assessing proposals on:
-
Collaboration strength
-
Scientific/methodological quality
-
Strategic alignment
-
Impact potential
-
Value for money
-
-
Panel review discusses reviewer feedback and agrees funding decisions.
Round 1 (2025)
Call launched (14 July) → Submission deadline (8 September) → Peer review (10 - 22 September) → Panel review (24 - 29 September) → Awards (2 October)
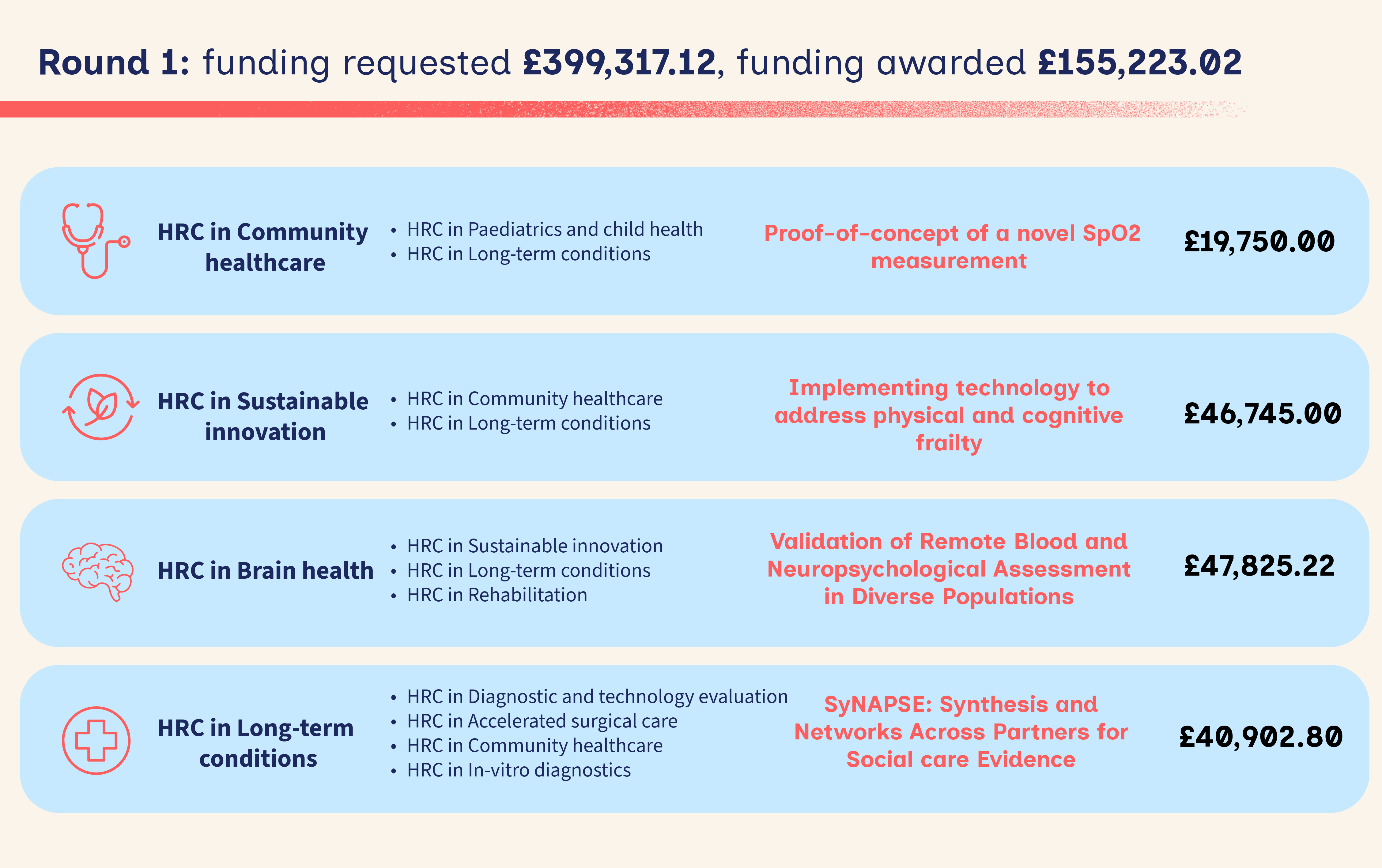
The first round demonstrated the breadth of research the CCF model can support. Round 1 saw all 14 HRCs engaged across applications and peer review. Nine applications were received (£398,967 requested), 4 projects were awarded (totalling £155,223). The projects commenced in November 2025 and will be completed by August 2026.
The 4 funded projects:
The amount of oxygen carried by your blood is a vital indicator of your overall health, measured everywhere from GPs to hospitals. Unfortunately, devices used to measure oxygen saturation struggle when a patient cannot be still, commonly leading to incorrect diagnoses or additional monitoring for children or people with tremors. This project demonstrates an oxygen saturation measurement that is resilient to patient movement which will improve accuracy of diagnoses and efficiency of care.
Frailty affects 1 in 10 people over 60, with 1 in 5 experiencing mild cognitive issues. No approved drug treatments exist, but non-drug approaches, improving muscle, cognition, sleep, and reducing stress, show promise. One emerging technique is transcutaneous vagus nerve stimulation (tVNS), which uses gentle electrical pulses via ear or neck devices. Early studies suggest benefits, but more research is needed. This project will unite experts across engineering, rehabilitation, aging and digital health to design a trial using tVNS. We’ll review evidence, hold expert meetings (including public contributors), and develop a trial plan, logic model, and funding application.
We need to improve how we monitor brain health in people as they age. 99% of people with early dementia symptoms are not assessed by a specialist clinic. New technologies could assess these people from home or through their GP. Computerised brain testing is very good at detecting early symptoms, and blood tests can now detect the early signs of dementia. We are working with a new blood sampling kit that uses a fingerprick of blood to test for these signs. Our early data shows that this approach is very accurate. This project will build on our work in this area. We will recruit 100 people with early cognitive impairment and 100 people with no symptoms, paying particular attention to making sure they are diverse in age, sex, location and ethnicity. They will complete a fingerprick blood sample and computerised brain testing from home. We will analyse this data to see whether this approach can accurately detect early brain changes, and whether this combination of tools could be used to detect dementia in people living at home. The three HRCs will work together to support recruitment and to analyse the outcomes. We will also combine our expertise to build a larger project for future funding.
SyNAPSE brings together universities and care organisations to improve how technology is used in older adult social care. Many past tech projects were not shared or evaluated properly, making it hard to know what works. We will gather missing evidence and build stronger links between HRCs, care providers, and tech developers. We aim to avoid repeating mistakes, support better decision-making, and help future innovations succeed. This will benefit older people, care staff, and researchers.
Round 2 (2026)
Call launched (12 January) → Submission deadline ( 27 March) → Peer review (30 March - 24 April) → Panel review (27 - April) → Awards (7 May)
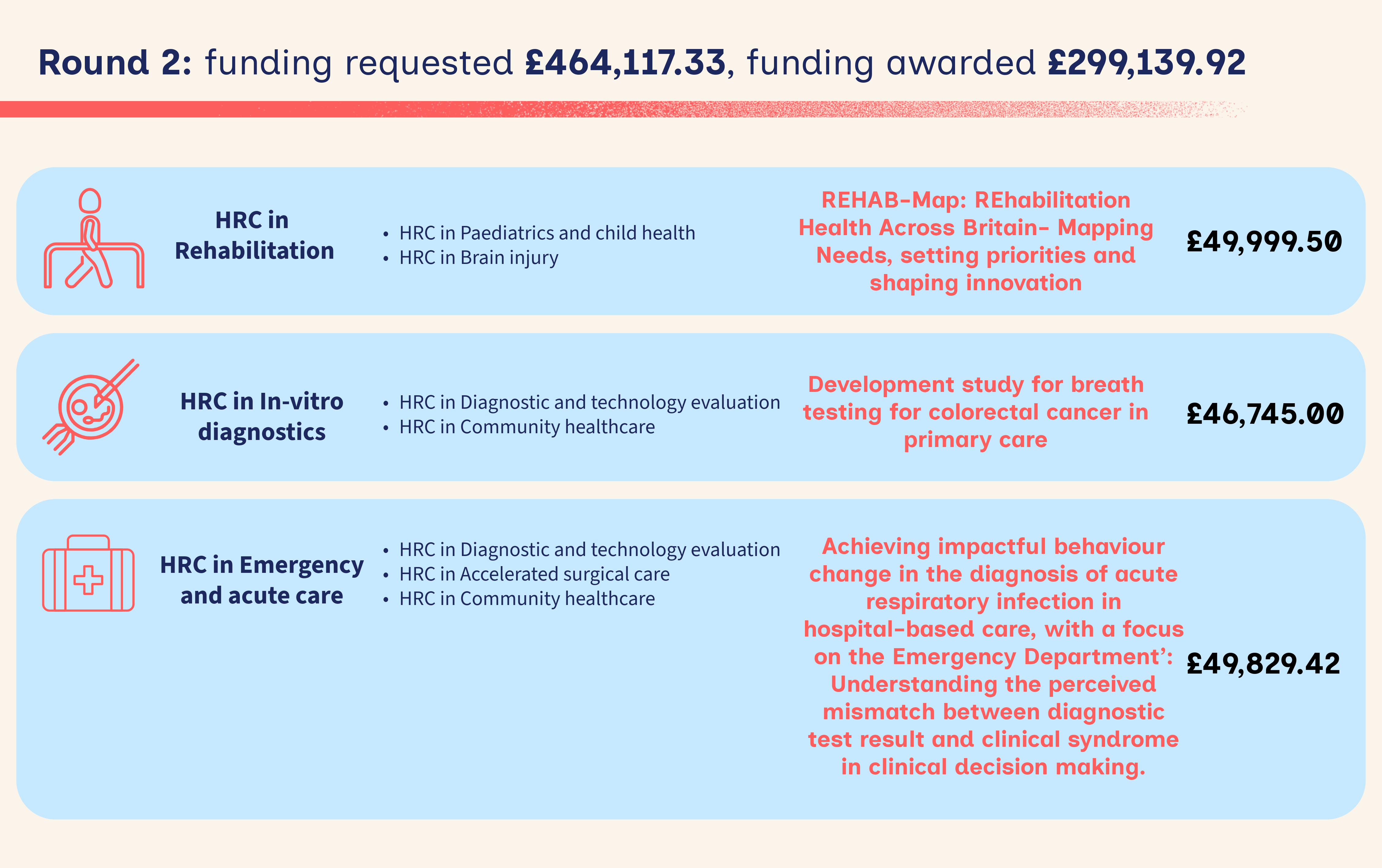
Round 2 achieved full engagement from all 14 HRCs engaged across applications. A total of 10 applications were submitted, requesting £464,117.33 in funding, with awards granted to projects totalling £299,139.92. The funded projects will begin in June 2026 and are scheduled for completion by March 2027.
The 6 funded projects:
Access to rehabilitation and opportunities to use technology to help the rehabilitation process is varied depending upon diagnosis and where someone lives. This project will better understand this and help us know what the most important questions for rehabilitation technology research are. Our national research group will map the rehabilitation and rehabilitation technology opportunities across England, making it clearer who the underserved communities are. We will talk to these communities to agree what are the most important research questions involving rehabilitation technology. We will publish those research questions, and the information collected along the way, so anyone can use them.
Each year in the United Kingdom there are 17,000 deaths related to bowel cancer. If diagnosed early, the majority of people survive bowel cancer. It is difficult to diagnose as symptoms are similar to other conditions. If a GP thinks a patient has bowel cancer they will refer them for a camera test, which can be an unpleasant experience. Only 3 out of 100 patients who have a camera test are found to have cancer. Stool (poo) based tests have been introduced but they are still unacceptable to some patients and the majority of patients with a positive test will be found not to have cancer. Our proposed solution is a simple breath test for patients with relevant symptoms. The breath samples are analysed for small molecules, which provide early indicators of bowel cancer, to identify those who would most benefit from a camera test.
Antibiotics treat and prevent bacterial infections but using them too often or in the wrong way makes them stop working. This is called antimicrobial resistance, and it’s a serious global health problem. When patients arrive at the emergency department within hospitals, healthcare professionals use tests to help decide if patients need antibiotics. Sometimes test results are hard for healthcare professionals to use, which can lead to antibiotics being given when they are not needed. To explore how to overcome these challenges, we will explore how healthcare professionals make these decisions and then share our work with patients and experts to develop ways to better support decision-making.
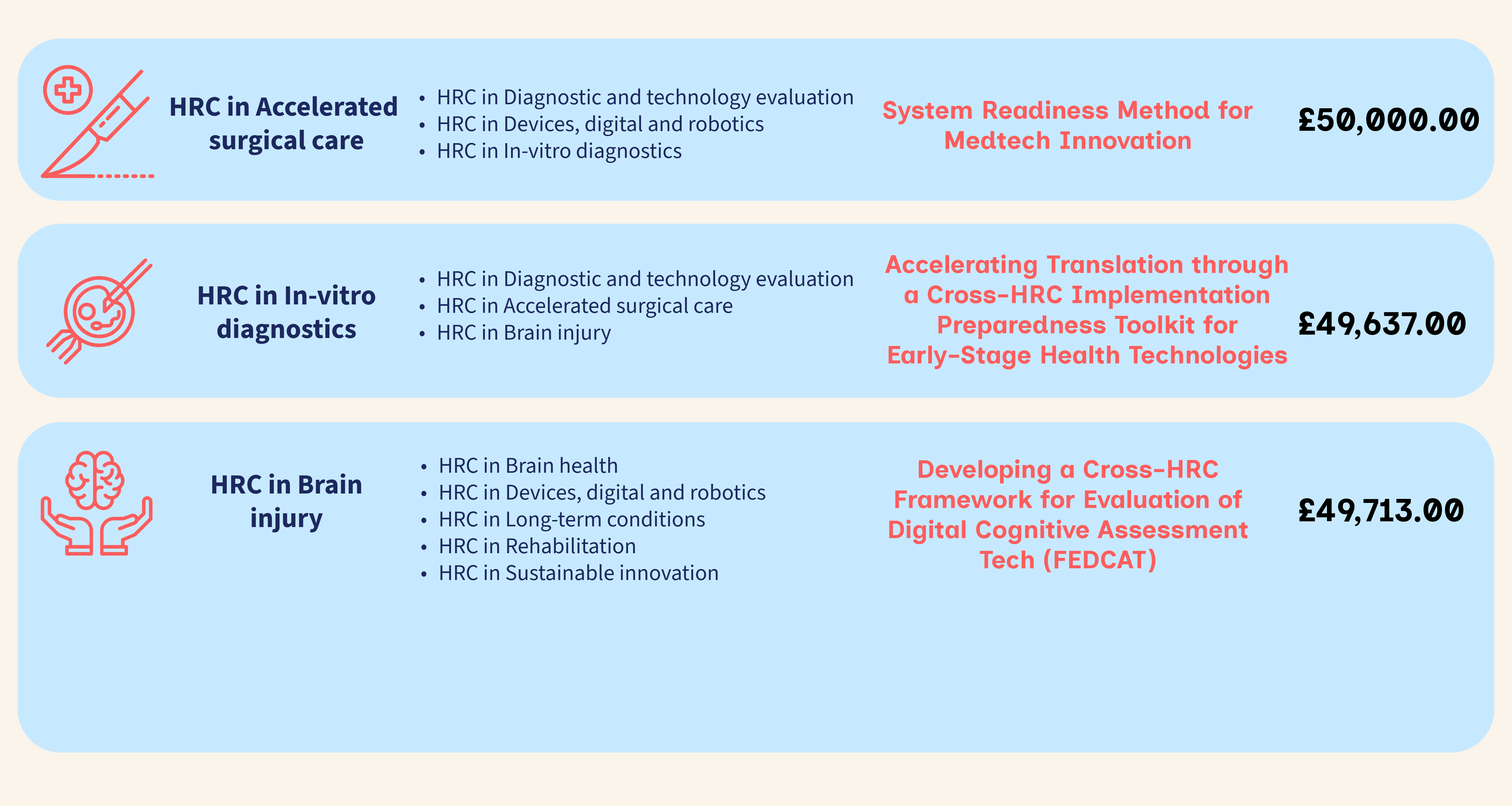
Despite significant investment in new medical technologies in the NHS, many of them still struggle to be used effectively in real NHS settings. The way we currently assess new technology does not consider how well it fits in real-world hospital environments, clinics and communities i.e. is the department/setting actually ready for the implementation of a new piece of technology? Most technology-based projects do not meet their goals, and very few recommended products are fully adopted in the most useful or valuable way. These failures waste money and miss chances to improve patient care. To address this, we will develop a method for better understanding this problem and predicting how much re-design of the technology or the setting is required to effectively implement the technology. Unlike current methods that focus mainly on the technology itself, this project will also consider the influences that staff, patients, hospital pressures, workflows and infrastructure have. The long-term goal is to develop a way to make these considerations a standard part of NHS decision making when choosing which technologies to invest in.
There are many cognitive assessment tools being developed by innovators to help people affected by dementia, stroke and other neurological conditions. However, there is a lack of validated tools to measure cognitive function at scale within routine clinical services. There is a lot of variation in the design, cognitive domain coverage, validation approaches and intended clinical use of existing solutions. There is therefore an opportunity to align the HRCs to reduce duplication and clarify what components constitute a robust, scalable and clinically meaningful digital cognitive assessment solution. This project will bring together clinicians, researchers, innovators and patient representatives across multiple HRCs. We will work to identify unmet needs in cognitive assessment and develop an evaluation framework. The outputs will improve coordination across centres and support the development of high-quality, scalable digital assessment solutions.
Health technologies (diagnostics, devices, digital/AI tools) are often developed with strong technical performance but limited preparation for NHS implementation. As a result, promising technologies frequently encounter barriers in practice, leading to delays, redesign costs and slower patient benefit. Implementation science offers structured methods to assess feasibility, acceptability, adoption and sustainability. However, existing frameworks are largely designed for mature technologies (TRL 7–9), with no clear guidance for early-stage development (TRL 1–4), where design decisions remain modifiable. This project will develop and pilot a cross-HRC Implementation Preparedness Toolkit for early TRL technologies. We will map existing tools to TRL stages, co-design structured guidance with stakeholders, and pilot the toolkit across early-stage projects in diagnostics, devices and digital/AI. The toolkit will enable earlier identification of implementation risks, improve design decisions, and accelerate translation into NHS practice.
Round 3 (2026)
The third round of the CCF will launch in Autumn 2026.