Each HRC has unique expertise to help you through your journey. However, all HRCs provide support to provide the necessary evidence to support your regulatory approvals.
Specialists in supporting HealthTech across the lifecycle
HRCs are experts in supporting innovators across the product lifecycle to ensure their products are developed safely and with patients at the centre.
While some innovations are funded by larger organisations developing them, the majority of new healthtech innovations come from small to medium sized enterprises (SMEs) or micro-organisations with fewer than 10 employees. In these instances, HRCs typically support the companies to secure the funding necessary to help them move their product along the lifecycle.
Evidence generation
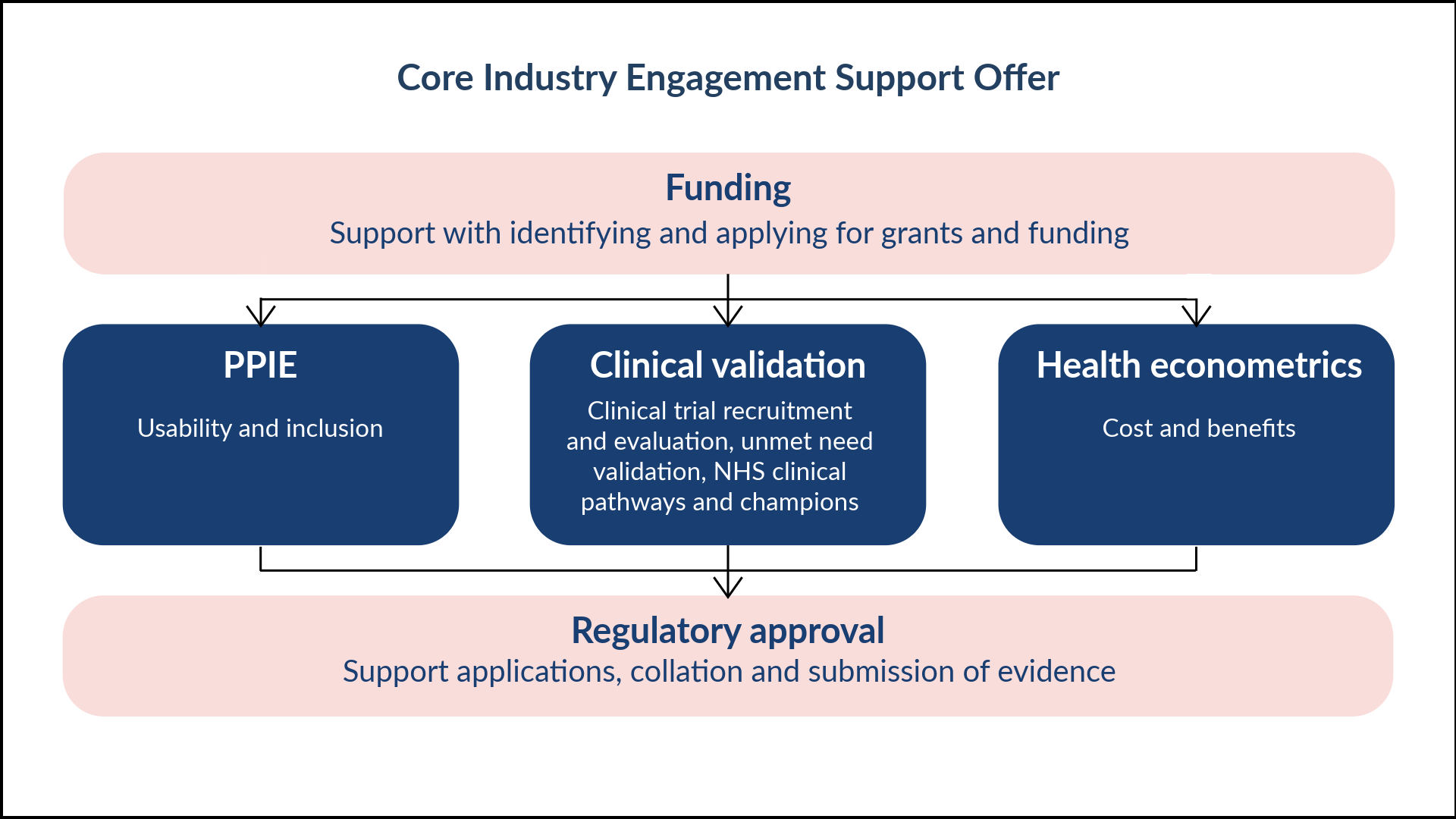
To apply for regulatory approval to get innovations adopted and used across the NHS, innovators must provide evidence to demonstrate that they have created an innovation that meets a clinical need, that has been developed and trialled with patients, and that demonstrates value to the NHS. Click below to find out more about what types of evidence HRCs can support innovators with.
Many funders now require a full PPIE integration strategy in recognition of the value it provides. From co-design and acceptability testing, through to interpretation of results and advocating for adoption, HRCs can support meaningful PPIE activities to improve the quality of your devices throughout the development process, enhancing your chances of successful adoption and implementation. Find out more here.
Unmet need can be quantified via the PICO (Population, Intervention, Comparator, Outcome) framework and considers the need from the NHS's operational budget and the patient's lived experience. Validation involves a formal Clinical Gap Analysis and Care Pathway Mapping to prove the technology offers relative effectiveness over the current standard of care. PPIE activities can help validate problems that matter to patients and carers, what aspects of the current care pathway fail them, and what frustrations shape their overall experience. For high-impact innovations, the Innovative Devices Access Pathway (IDAP) or Early Value Assessment (EVA) provide formal Unmet Clinical Need Authorisation, which serves as the official green light for targeted evidence generation.
Clinical investigations specifically refer to studies involving medical devices. They are governed by the Medical Devices Regulations (UK MDR 2002) and, for those aiming for Northern Ireland or EU markets, the MDR (EU) 2017/745. They focus on the physical, mechanical, or software-driven performance of a tool used for diagnosis, monitoring, or treatment. Recruitment is strictly validated through Patient and Public Involvement and Engagement (PPIE) to ensure investigation designs are inclusive and feasible for underserved populations, a legal expectation under the new transparency and diversity mandates.
Care pathways are aligned to medical conditions and describe a patient’s journey across an episode of healthcare. Care Pathway Analysis (CPA) maps the processes and method for modelling a care pathway in a healthcare system and is used to assess the impact of bringing a new innovation into the clinic, to understand how their product will fit in and potentially change the current pathway. CPA is an important part of the early evaluation process as it helps identify problems in current pathways and the optimal role and place of the new innovation, and the optimal patient population to use the innovation with.
This helps innovators to understand which characteristics of their device would be clinically feasible and acceptable by providing clarity on who the technology is for, what problem it solves, and why it matters. A clear business case shows how these benefits translate to cost savings or health improvements, and can be translated into measurable outcomes for clinical studies, such as time-to-diagnosis, correct referral rates, and clinician time saved. This important work can support regulatory applications, determine clinical outcome measures for a future trial, inform R & D strategies, demonstrate commercial viability and plausible routes to adoption.
Health economics is the study of how healthcare resources are allocated, how much interventions cost, and what value they deliver in terms of health outcomes. It helps compare different tests, treatments, and pathways to determine which options provide the best results for the resources invested. Early health economics studies are performed earlier in the development process with an aim to explore potential cost-effectiveness, steer investment decisions, and identify key aspects of the care pathway that drive value. A full economic evaluation will assess the value of a device in a real-world setting, supporting reimbursement, pricing and policy decisions. A comprehensive economic model is required for NICE evaluation.
Regulatory support
There are many different routes to regulatory approval depending on the type of innovation, and where the innovation will be used. HRCs are experts in guiding innovators to ensure they get the right regulatory approvals to enable them to get their innovation to market and to patients.
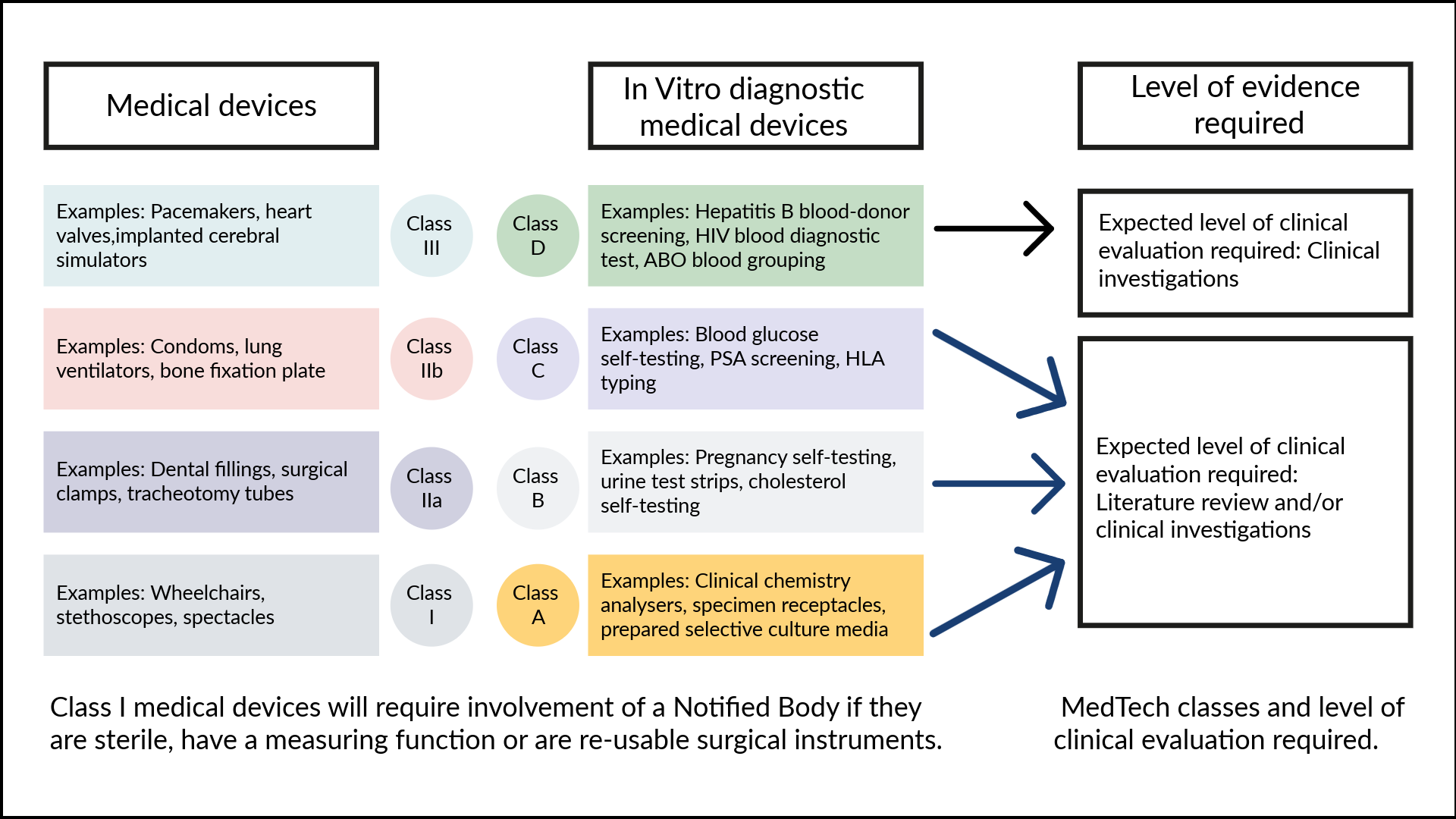
Regulatory classifications
In the UK, healthtech products are classified by the MHRA under the UK MDR 2002 (as amended) based on a tiered, risk-based system that determines the level of regulatory scrutiny required. For software-as-a-medical-device (SaMD) and AI, recent 2026 updates are shifting most diagnostic or treatment-influencing tools out of Class I and into Class IIa or higher, requiring mandatory assessment by a UK Approved Body.
CE and UKCA regulatory markings
While the UKCA mark remains a valid and available domestic route, the MHRA proposes that devices compliant with the EU MDR and IVDR can be placed on the market without a separate UK certification, a move intended to protect patient access to the 90% of healthtech products currently imported from the EU. Under existing transitional arrangements, CE-marked devices remain legally accepted until at least 2028 or 2030 (depending on the device class), but the new 2026 proposals aim to remove these sunset dates entirely, repositioning the UKCA as a specialized innovation route for first-in-market technologies like AI-as-a-medical-device (AIaMD).
NICE evaluates and develops guidance for healthtech to improve the uptake of devices and technologies in the NHS, particularly those that deliver treatment (e.g., surgical implants), give greater independence to patients, or detect and/or monitor medical conditions. Their guidance is based on the stage that an innovation is currently at and NICE often group healthtech products that have a similar use, or address a similar need. They can make a recommendation for the use of the approved innovation with guidance on how it should be used, not used or used only in specific conditions (such as managed access periods, or for research). They also provide recommendations on using certain innovations over other similar technologies in use in the NHS, and what to consider when choosing between these technologies.
The Medicines and Healthcare products Regulatory Agency (MHRA) acts as the UK’s executive "gatekeeper" and safety supervisor for all medicines, medical devices, and blood components. Its primary mandate is to protect public health by ensuring that healthcare products meet rigorous standards of safety, quality, and clinical performance before they reach the market and throughout their entire lifecycle. They authorise clinical trials and investigations, certify high-risk devices, and manage the Yellow Card scheme for reporting adverse incidents and accelerate access to Software-as-a-Medical-Device (SaMD) and AI-as-a-Medical-Device (AIaMD).